
Facing surgery for Inflammatory Bowel Disease (IBD) can feel like a daunting turning point. For many, it's not the first choice, but rather the solution when biologics and steroids stop working. Whether you're dealing with Crohn's disease a chronic inflammatory condition of the gastrointestinal tract that can affect any part of the digestive system from the mouth to the anus or Ulcerative Colitis an inflammatory bowel disease that causes long-lasting inflammation and ulcers in the innermost lining of the large intestine and rectum, the goal of surgery is the same: getting your life back. While the idea of a "stoma" or "removing a colon" sounds scary, modern techniques are focused on preserving as much bowel as possible and minimizing the time you spend in a hospital bed.
The reality is that surgery is common in the IBD community. About 75% of people with Crohn's and up to 30% of those with ulcerative colitis will need a procedure at some point. It isn't a failure of treatment; it's a different tool for a different stage of the disease. From resolving a dangerous blockage to eliminating the risk of cancer, these procedures can shift you from surviving to actually thriving.
Key Takeaways for IBD Surgery Patients
- Resection is common for Crohn's to remove damaged segments while keeping the rest of the bowel.
- IPAA (J-Pouch) is a gold-standard for ulcerative colitis, allowing most patients to avoid a permanent bag.
- Ostomies can be temporary (to let the bowel heal) or permanent (if the rectum is removed).
- Recovery involves a learning curve of 6-12 months for pouch function and specialized care for skin health.
- Success rates are high, with 80-90% of J-pouch patients reporting high satisfaction.
Understanding Bowel Resection and Colectomy
When doctors talk about Resection the surgical removal of a part of an organ or structure, in this case, a section of the intestine, they are talking about cutting out the "bad" part of the gut and sewing the healthy ends back together. In Crohn's disease, this is often a segmental resection. Instead of taking out the whole organ, surgeons target specific areas of inflammation or strictures (narrowing of the bowel) that cause blockages.
For those with ulcerative colitis, the focus often shifts to a Colectomy the surgical removal of all or part of the colon. Since ulcerative colitis only affects the large intestine, removing the colon effectively removes the disease from the body. Many of these procedures are now done laparoscopically, which means smaller incisions and shorter hospital stays-often reducing your time in the ward by a couple of days compared to traditional open surgery.
If the disease has spread to the rectum, a proctocolectomy is required. This is where the surgeon removes both the colon and the rectum. Depending on your health and the state of your anal sphincters, this leads to two primary paths: a permanent ostomy or the creation of an internal pouch.
The J-Pouch: IPAA and How It Works
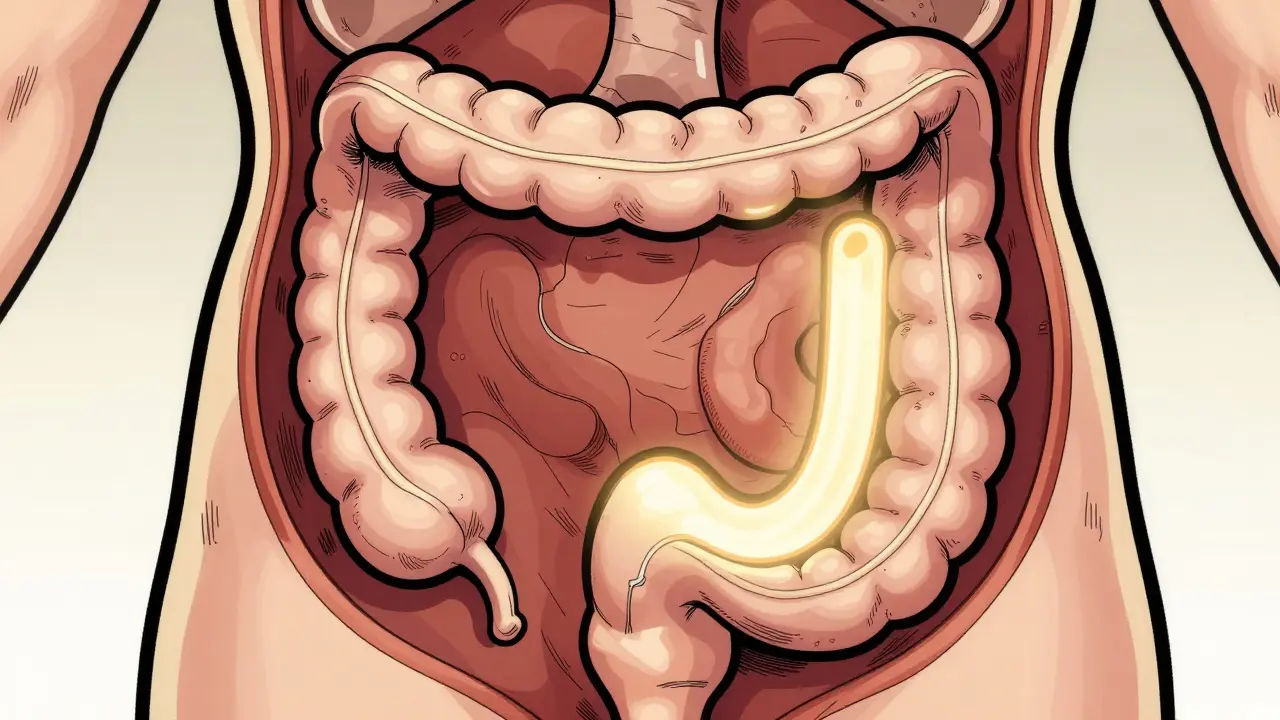
The Ileal Pouch-Anal Anastomosis a surgical procedure where the end of the small intestine is shaped into a pouch and connected to the anus to replace the removed colon and rectum, or IPAA, is a game-changer for ulcerative colitis patients. Essentially, the surgeon uses a piece of your remaining small intestine (the terminal ileum) to create a reservoir, or "pouch," that holds waste until you're ready to go to the bathroom. This is the "J-pouch" because it's often shaped like the letter J.
This is rarely a single-step process. Most patients undergo a three-stage journey to ensure the pouch heals correctly. First, the colon is removed and a temporary ileostomy is created to divert waste. About 8 to 12 weeks later, the pouch is constructed. Finally, once the pouch is confirmed to be leak-free, the temporary ostomy is reversed. While this sounds like a lot of time in the OR, it significantly lowers the risk of life-threatening leaks, which happen in about 5-15% of these cases.
| Procedure | Best For | Main Goal | Outcome |
|---|---|---|---|
| Segmental Resection | Crohn's Disease | Remove blockages/strictures | Symptom relief; risk of recurrence |
| Total Proctocolectomy | Ulcerative Colitis | Remove all diseased tissue | Disease elimination; requires ostomy or pouch |
| IPAA (J-Pouch) | Ulcerative Colitis | Maintain natural bowel habits | Continence in 80-90% of patients |
| Strictureplasty | Crohn's Disease | Widen narrowed bowel | Bowel preservation; avoids "short bowel" |
Living with an Ostomy: Temporary and Permanent
An Ostomy a surgically created opening in the abdominal wall to divert waste from the body into a pouch is often a source of anxiety, but for many, it's the first time they've felt safe leaving the house in years. A stoma is essentially a small piece of bowel brought through the skin of the abdomen. For an ileostomy, this is usually about the size of a quarter.
Whether your ostomy is temporary (like during the IPAA process) or permanent, the daily management is similar. You'll use a specialized bag that adheres to your skin. Most people find they need to empty these bags 4 to 6 times a day. The biggest hurdles aren't usually the bag itself, but skin irritation and body image. Pro tip: invest in a high-quality ostomy belt to keep the bag secure and prevent leaks, especially if you're active.
For those over 65, a permanent ostomy is often preferred over a pouch. Why? Because the risk of complications with a pouch is higher in older adults, and a permanent stoma completely eliminates the risk of colorectal cancer, which is a major concern for long-term IBD patients.
Postoperative Care and the Road to Recovery
Recovery doesn't end when the stitches come out. If you've had a J-pouch, you're looking at a learning curve of 6 to 12 months. Your body needs to "learn" how to use the new reservoir. Initially, you might have 6 to 10 bowel movements a day, but this usually settles down to 4 to 8 over time.
Hydration is your new full-time job. Because the colon-which normally absorbs water-is gone or altered, you need to drink 8 to 10 cups of fluid daily to avoid dehydration. Be careful with high-fiber foods in the beginning; things like popcorn or raw broccoli can cause blockages in a newly fashioned pouch or stoma.
You also need to watch for "pouchitis," an inflammation of the pouch that affects up to 40% of IPAA patients. If you notice a sudden increase in bowel movements, mucus in the stool, or a fever over 38.3°C (101°F), get in touch with your team immediately. Most pouchitis is easily managed with a course of antibiotics.

Managing the Emotional and Physical Transition
Surgery is as much a mental game as a physical one. Many patients report a huge sense of freedom-no more "bathroom anxiety" or blood in the stool. However, the transition to a stoma can be hard. It's common to feel a loss of control over your body initially.
The best way to handle this is to connect with a certified wound ostomy continence nurse (WOCN) before the surgery even happens. They provide the hands-on training you need to master the appliances. Additionally, communities like the United Ostomy Associations of America provide a space to realize you're not alone in this. Whether it's finding the right adhesive or dealing with nighttime seepage, there's almost always a veteran patient who has a trick to help.
Will I always have a stoma bag?
Not necessarily. If you have a temporary ileostomy as part of a J-pouch procedure, the bag is typically removed after 8-12 weeks once the internal pouch has healed. However, some patients require a permanent ostomy if the rectum cannot be preserved or if the anal sphincter doesn't function correctly.
What is the success rate of J-pouch surgery?
The long-term outlook is quite positive. Around 80-90% of ulcerative colitis patients report high satisfaction and maintain continence. Long-term pouch survival rates are estimated at 90% over a 10-year period, though some may need minor adjustments for pouchitis.
Can I eat normally after IBD surgery?
Eventually, yes, but there's a transition period. Initially, you'll need to avoid high-fiber, "stringy" foods (like celery or nuts) that could cause a blockage. Over time, most people return to a varied diet, though increasing fluid intake becomes a lifelong necessity to prevent dehydration.
Does surgery cure Crohn's disease?
Unlike ulcerative colitis, where removing the colon removes the disease, Crohn's can appear anywhere in the digestive tract. Surgery treats the complications (like strictures or fistulas) and can lead to remission, but it isn't a total cure. Recurrence rates can be high, which is why maintenance therapy usually continues after surgery.
What are the risks of IPAA for women and men?
There are specific risks associated with the pelvic dissection during pouch surgery. Men face a 15-20% risk of new-onset erectile dysfunction, and women may see an increase in infertility rates (from 15% to 50-70%). These are important conversations to have with your surgeon beforehand.
Next Steps and Troubleshooting
If you're currently deciding on surgery, your first step should be a consultation with a colorectal surgeon who specializes in IBD, rather than a general surgeon. Dedicated IBD teams have been shown to reduce complication rates by up to 35%.
For those currently recovering:
- Skin Issues: If your skin is itching or peeling around the stoma, try a barrier ring or powder. Don't let the skin get raw; see your WOCN for a fitting adjustment.
- Hydration: If you feel dizzy or have dark urine, increase your water intake and consider electrolyte replacements.
- Pouch Function: If you're having 10+ movements a day after the first six months, ask your doctor about pouchitis or a potential diet trigger.


william wang
The point about IBD-specific surgeons is huge. I've seen a massive difference in outcomes when you go to a specialist who does nothing but these pouches and resections all day versus a general surgeon who might only do one a month.